Today’s tip is about a subtle but game changing technology. Do you know what a variable working distance is on your loupes?
As many of you know, I tried out multiple brands of ergo prism loupes at the same time, and switched to ergo prism loupes.
It’s been an incredible game changer. My neck pain is gone and my pinched nerve symptoms have almost all gone away in a matter of months!
I want to talk about a feature Lumadent’s loupes have that the other brands of loupes did not have.
Variable Working Distance
So the thing Lumadent has that the other brands I tried did not have is a variable working distance. This is a VERY AWESOME feature.
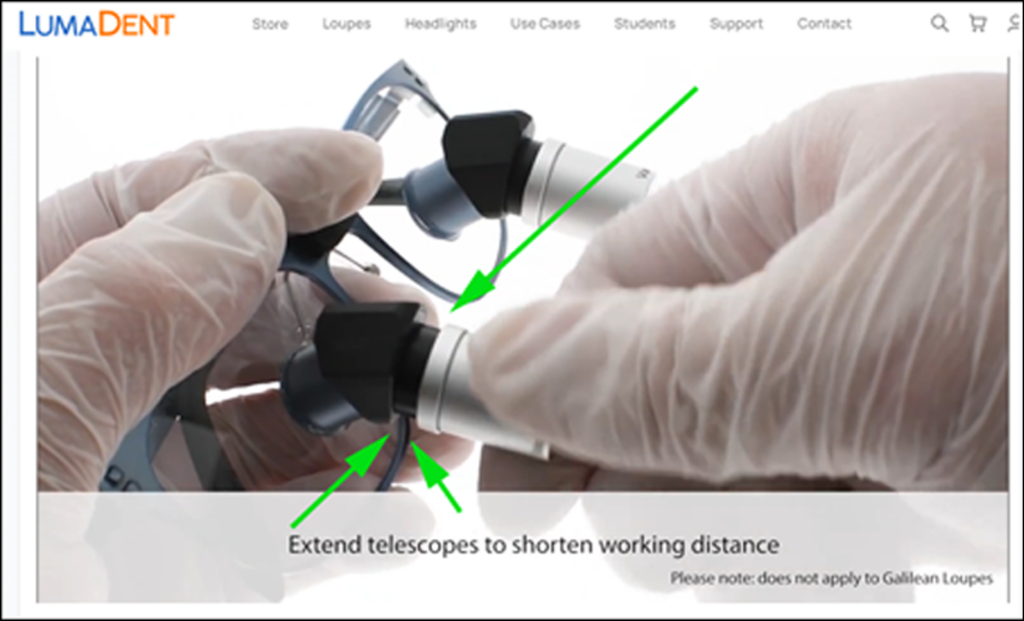
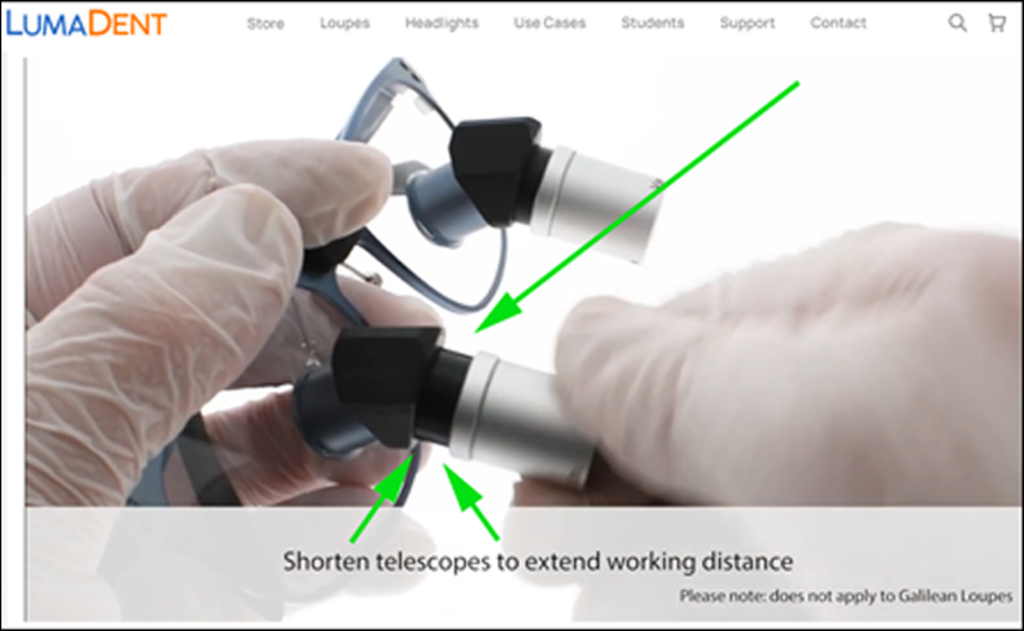
In short, you can turn each loupe lens like binoculars to change the working distance. YOURSELF.
It works by simply turning the focus on the lens clockwise or counter-clockwise, depending on if you want to shorten or lengthen your working distance.
Here is an example of how adjusting the working distance works:
They also have a good video that shows this here at the 2 minute mark:
The range is impressive. It’s around 12 inches of ADJUSTABALE working distatnce. But the range changes with each magnification.
I’ll tell you why this is so important. There are two reasons:
Fine tuning (reason #1)
The first is fine tuning. I know when you buy loupes the rep gets you all measured up with working distance, but my question is how do you really know?
I remember watching the sales rep in dental school almost have an assembly line of students, slamming almost everyone into a 16-inch working length but that never made sense as there were 5’4″ students and 6’2″ students, but everyone seemed to be getting 16 inches because that was the average.
Well, I know I got my working length at 21 inches, and sent them back twice,ultimately settling on 23″ working length.
The idea is you want your loupes to put you in the position that is most ergonomically comfortable to your body.
Your loupes are NOT supposed to put your body in a non-ideal position that is not ergonomically ideal to your body.

The point I’m making is your sales rep can (should?) get your working distance close. But do you really know? I don’t.
In my personal case, after trying Lumadent’s ergo loupes, I learned I like to sit my patient lower than I anticipated. Instead of sending my loupes back, waiting 6+ weeks, I simply turned some dials, played around a little bit, and got my loupes / patient positioning into a more comfortable position. Took m a few days, but I got my patient positioning really dialed in, and a BIG reason why I feel my back and neck pain has gone away.
So having that ability to fine tune your working distatance an additional 10-12 inches AFTER you get your loupes is a game-changer.
And this game changer does NOT go away. Which leads me to my second point.

Long-Term (reason #2)
The variable working distance is an incredible hedge.
While Lumadent’s pricing was the most affordable of the ergo loupes brands I tried (by over $1,000) changing loupes when eye prescription changes is EXPENSIVE.
Even if you do not wear corrective lenses, it is well known eyes change around 40-45 years old. Especially with all the time spent on smart phones and computers in this modern age.
I checked with my optometrist friend and he confirmed that due to the loupe’s high magnification if my glasses prescription changes I can simply change my working distance on my loupes and that should be sufficient.
So having Lumadent’s variable working distance feature it also helps protect against eyeglasses prescription changes.

Two questions:
Now I get asked two questions a lot, and I admit I had the same questions myself.
People often ask me about the weight of the loupes. While they look heavy, ergo prism loupes are NOT heavy. In fact my Lumadent loupes are the lightest loupes I have ever worn.
The other question I get asked a lot is does it take a long time to adjust to ergo prism loupes? For me it was 2-3 days and by the end of the week I was fully dialed in.
What I recommend when switching to ergo prism loupes is to start off only doing hygiene recalls and occlusal fillings. Stick to simple stuff at first. But I found it easy and a quick process to adjust to ergo loupes.
Summary
So the reason why I am going into such depth on a variable working distance is because I do not think a lot of people are aware of. I actually bought my Lumadent loupes NOT even knowing I could adjust my working distance. And Lumadent was the ONLY loupe brand I tried out that had this feature.
So in short, a variable WD lets you accomplish two things:
(1) you can fine tune your ergonomic position AFTER you get your loupes to be even MORE dialed in for a better ergonomic position.
(2) you save money on future prescription changes, by being able to adjust your working length.
Complete game changer. I think every dental student and every dentist should be in ergo prism loupes. It is my opinion these loupes help save backs in pain on seasoned dentists, and prevent neck pain from happening in dental students.
I know I’m glad I switched.
Click here to learn more about Lumadent ErgoPrism Loupes today.
I hope these tips are helping.
To your success,
Dr. Greg (aka “The Helpful Dentist”)